This blog was first published in Brookings Future Development Blog. The authors are Ipchita Bharali, Preeti Kumar, and Sakthivel Selvaraj.
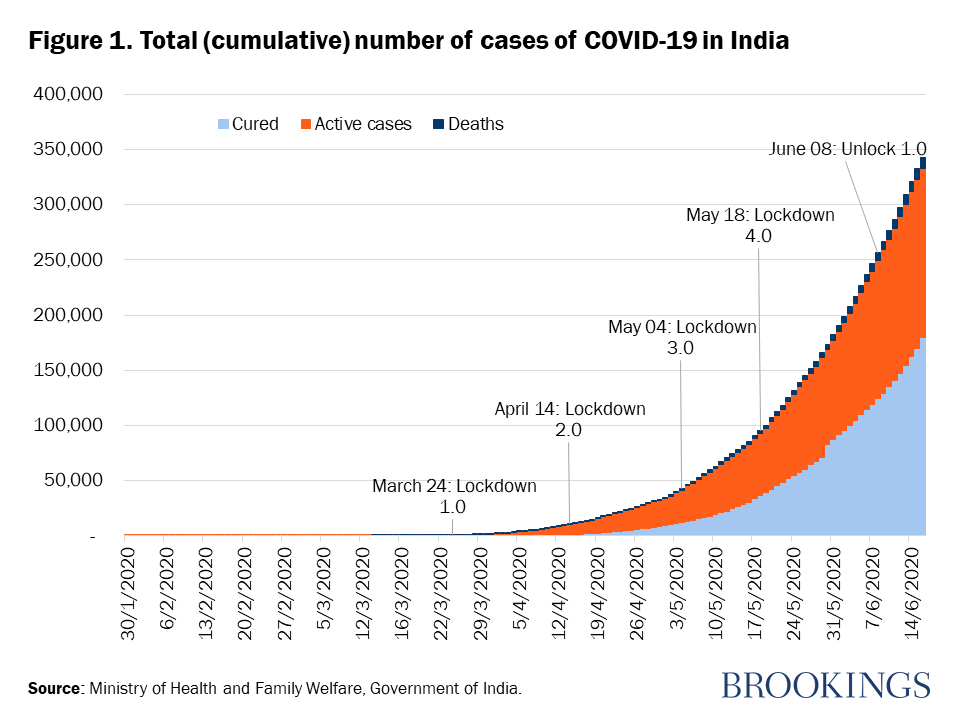
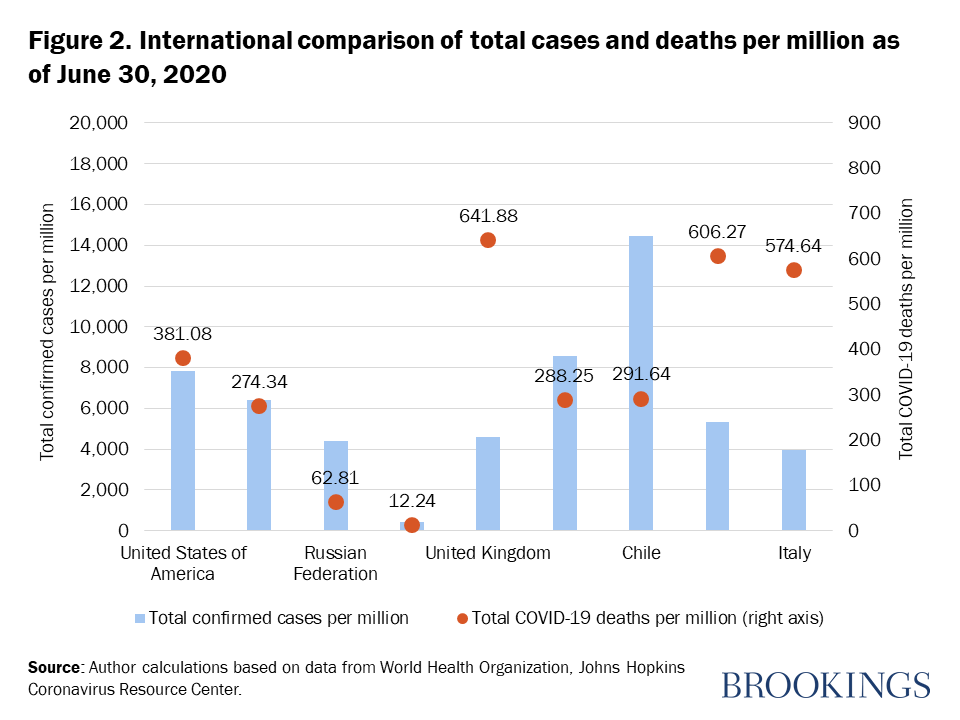
The first COVID-19 case in India was detected on January 30, the same day that WHO declared it a public health emergency of international concern. India went into lockdown almost two months later. On June 8, after 10 weeks of lockdown, India started a phased reopening of its economy. With Unlock 1.0, the country is trying to balance attempts to revive the economy while dealing with increasing caseloads and new hotspots. On June 30, official COVID-19 cases stood at over 585,000, and more than 17,500 deaths (Figure 1). While recovery rates have improved to 60 percent and the death rate is relatively low considering that India is the fourth most-impacted country globally, COVID-19 in India is nowhere close to the peak (Figure 2).
Recent analysis done jointly by Duke University’s Center for Policy Impact in Global Health and the Public Health Foundation of India assesses India’s pandemic preparedness and its policy response has been varied across the states. It also provides a snapshot of the current situation. But its main contribution is to identify the policy gaps that India must close quickly.
National weaknesses: Low testing rates, deteriorating health care, and poor social protection
India alertly implemented surveillance as early as January 17, even before the first cases were officially detected. This was followed by a series of travel advisories and restrictions, and efforts to repatriate and quarantine Indian nationals arriving from abroad. But low testing rates have always been a serious drawback. When the curfew and lockdown were imposed, only 6,500 samples had been tested nationwide, and the daily testing capacity in mid-March was just 1,400 samples. Testing capacity has increased in recent weeks—over 1,000 laboratories with daily testing capacity of more than 300,000 samples—but testing rates are still low. According to the FIND database from June 14, India tests around 4,100 people per million compared with a global average of over 29,000 tests per million.
After a 14-hour “Janata Curfew” test run, India went into full lockdown on March 24; at the time, India had just 500 confirmed COVID-19 cases and fewer than 10 deaths. The sudden lockdown had a severe impact on millions of low-income migrant workers and daily-wage earners. With no savings and little guidance or financial help from the government, these workers and their families faced food insecurity and hardships that led many to walk hundreds of miles to reach their villages. News of migrants killed in road and train accidents made headlines, along with reports of migrants fleeing quarantine centers due to overcrowding and unhealthy facilities. The economic impact of the lockdown on migrants was mitigated through provision of rations by the government, but this was implemented more than 45 days after lockdown.
Migrant flight has serious implications on the already fragile rural health infrastructure. It is estimated that between 2 million and 10 million migrants were impacted by COVID-19. A severe impact on other health programs due to COVID-19 is also evident from the analysis of the National Health Mission data on inpatient and outpatient treatment. Between 100,000 and 200,000 children missed routine vaccinations during February and March. Treatment for tuberculosis also showed declines.
These data do not capture services provided by the private sector, which accounts for 70 percent of health care provision and half of hospitalizations in India. Analysis conducted on the claims data of the flagship Pradhan Mantri Jan Arogya Yojana insurance program, which was launched to provide financial protection to the poorest households, also showed that weekly claims volume during the 10 weeks of lockdown was half the pre-lockdown claims volume. Claims for cataract eye surgery and joint replacements fell by over 90 percent, and significant declines were also seen in cardiovascular surgeries, child delivery, and oncology. These findings raise concerns about a potential resurgence of vaccine-preventable illnesses, infectious diseases, and chronic ailments.
Big differences among states—and little convergence
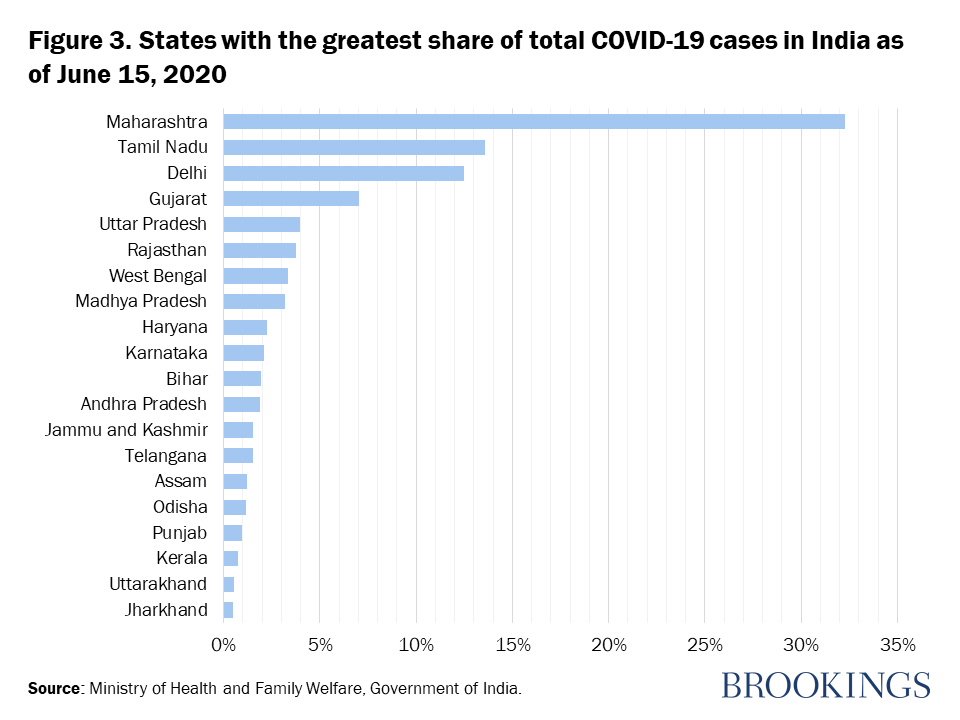
Given the key role of state governments in India’s health system, the response in India needs to be understood from a state level perspective. Currently, more than half of all COVID-19 cases are concentrated in three states: Maharashtra, Tamil Nadu, and Delhi (Figure 3).
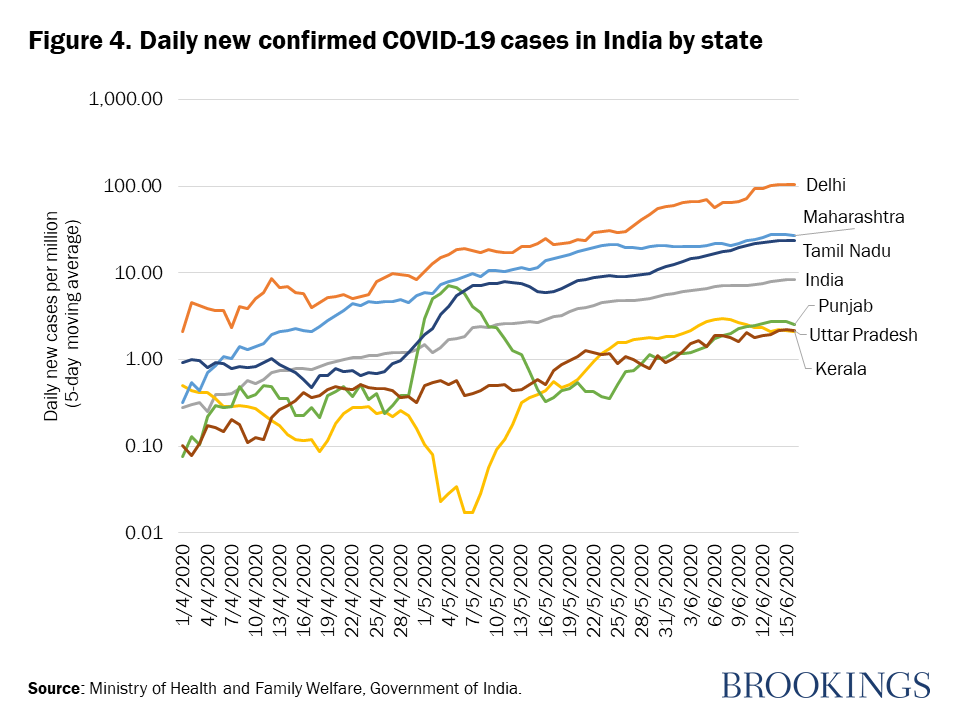
The daily new cases are also highest among these three states (Figure 4). While daily cases fell sharply in Kerala before increasing, it was the exact opposite in Punjab. This corresponds to when interstate movement of migrants was officially allowed beginning April 29. Although the first COVID-19 cases were detected in Kerala among a group of students returning from Wuhan, China, the state government’s COVID-19 response has been effective, with the state accounting for less than 1 percent of total confirmed cases in India. Kerala has received accolades from the U.N. for the COVID-19 response strategies it adopted . The state’s investment in public health care and experience tackling the Nipah outbreak in 2018 may have contributed to its capacity and preparedness to swiftly handle the current outbreak.
Data on testing rates across India show that most states need to ramp up testing (Figure 5). The bubble size in Figure 5 represents cases per million population. On June 15, the average testing rate in India was 4,972 per million. Ladakh had the highest testing rate at 38,170 per million, followed by Goa (27,568 per million), Jammu and Kashmir (20,400 per million), and Delhi (14,693 per million).
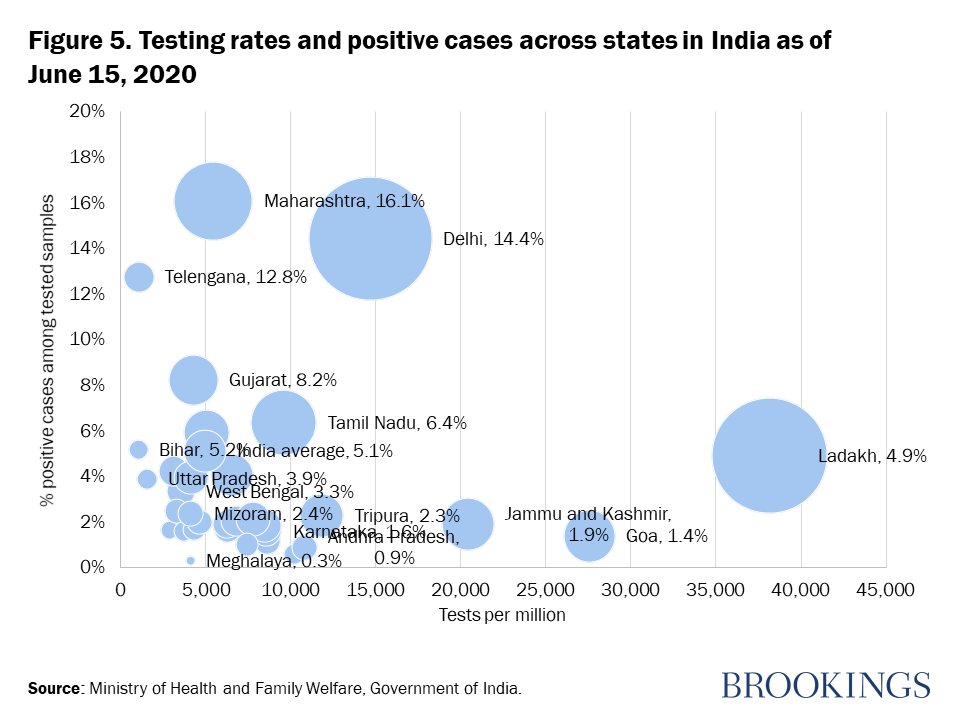
Maharashtra—essentially India’s New York state that has Mumbai, India’s financial center—accounts for almost a third of all cases. But it has a much lower testing rate of 5,445 per million compared with many other states, so the high number of cases in Maharashtra is not explained by a high test rate. States like Telangana, Gujarat, and Tamil Nadu have low testing rates coupled with a high percentage of infections. By increasing testing rates, these states will likely identify many more positive cases, which will help to isolate people and control spread. Kerala’s experience shows that testing needs to be complemented by effective contact tracing, isolation, and quarantine measures to effectively tackle the spread of infections.
India’s health capacity and policy gaps
Outside health policy, India’s weak economic response is a big problem. The Atmanirbhar Bharat (“Self-reliant India”) stimulus package announced in May is not small at $110 billion; this is equivalent to 10 percent of India’s GDP. But it comprises mostly monetary interventions to provide liquidity with a longer-term outlook to boost the economy. In terms of funding responses and relief measures targeted at the poor and vulnerable, the $23 billion Pradhan Mantri Garib Kalyan Yojana relief package falls short as it mostly reallocates funding across existing budgets or allows people to make advance withdrawals on their social benefits rather than mobilizing additional funding. India needs to do more to help the families of low wage workers displaced from their jobs by the lockdown and the weakening economy.
For the health sector, our analysis points to three main problems: low levels of testing, implementation failures in containing the spread during lockdown, and serious impacts on other health services. India’s response is consistent with its 2019 scores on the Global Health Security Index. In terms of health security—pandemic preparedness and capacity—India is ranked 57th out of 195 countries. Its score of 46.5 was above the global average of 40.2, but much lower than Asian middle-income peers such as Indonesia and Thailand that had scores of 56.6 and 73.2, respectively. India scores high on communications with health care workers during a public health emergency, trade and travel restrictions, laboratory systems, immunization, and socioeconomic resilience. But it does less well in zoonotic disease prevention, emergency preparedness and response planning, capacity of health facilities, health care access, and medical countermeasures and personnel deployment.
The full scale of policy responses needed to combat COVID-19 is still unclear because the outbreak has not yet reached its peak. In the longer term, what is required are investments in health infrastructure, ensuring continuity of regular health services, and improving health emergency preparedness. India will have to cautiously adjust spending, attract industrial investments to spur growth, and address rising unemployment. But over the next year, India can expect to remain in crisis mode. Based on the current status of COVID-19 and the lessons from its early response, India ought to be prioritizing five measures:
- Increase testing capacity. India can do this quickly by harnessing the capacity of the private sector for laboratories, test kits, and supplies. But the government will also have to increase the density and capacity of test sites and laboratories and improve procurement and supply chains. India’s domestic PPE kit production has been a great success story, which provides reasons for optimism.
- Assist poor workers. Steps to help poor migrant workers include programs offered by the Ministry of Housing and Urban Poverty Alleviation in their 2017 report. These policies include provision of affordable housing, emergency employment schemes, and access to social entitlements and service provisions. The recent announcement on provision of essential food supplies to 800 million people is a step in the right direction.
- Maintain regular health services. Maintain essential critical health services and disease programs to avoid a resurgence of vaccine preventable diseases, infectious diseases, and chronic illnesses. Both the central and state governments should look to expand strategic investments and partnerships with the private sector, development partners, and community health workers to strengthen surge capacity and ensure continuity of health provision.
- Enforce emergency measures. Enforce sensible social distancing, effective quarantine procedures, mandatory mask-wearing and hand hygiene habits, along with improved detection, containment, and mitigation.
- Enable responsible monitoring. Introduce and ensure national data privacy laws to improve India’s health emergency response and safeguard against data privacy concerns.
About the Authors:
Ipchita Bharali (tweets @IpchitaBharali) is a Policy Associate at the Center for Policy Impact in Global Health, Duke Global Health Institute.
Preeti Kumar, Vice President, Public Health System, Public Health Foundation of India.
Sakthivel Selvaraj, Director and Professor, Health Economics, Financing and Policy Division, Public Health Foundation of India.