Our Policy Associate, Kaci Kennedy McDade, attended the 2019 World Health Summit in Berlin. This blog is her reflection on the Summit.
At the World Health Summit last month, I attended a session on finishing the last mile of polio eradication. At the session, panelists described the remarkable gains that have been made over the last three decades. For example, since the launch of the Global Polio Eradication Initiative (GPEI) in 1988, poliovirus cases have decreased by over 99% and polio remains endemic in only three countries (Afghanistan, Nigeria, and Pakistan).
Although we have not yet achieved global polio eradication, a key topic of the discussion that may have surprised some attendees was transition. By transition, I mean the phase-out and withdrawal of polio-focused support. While some participants may have been concerned that transitions mean “shutting down” before we’ve “finished the job,” I welcomed the proactive discussion. In the era of sustainability, shouldn’t we be focusing on the future?
After all, donors have always touted their interest in “putting themselves out of business.” While to some, that may have seemed a scenario far off in the distant future, it is becoming a reality for many countries, particularly lower-middle income countries.
Why were some panelists concerned about GPEI transition? First, it’s a $1 billion annual funding portfolio concentrated in 16 countries. That’s a lot of money that could potentially exit the global health aid space.
Second, the panelists reminded the audience that polio funding, although considered a “vertical” program, has oftentimes targeted areas of the health system beyond strictly polio (referred to by the panelists as “polio assets”). For example, 25-50% of staff funded through GPEI actually support broader health programs including routine immunization, disease surveillance, and laboratory support. Once polio is eradicated and polio-centric funds are pulled, other areas that polio has historically supported could suffer.
Third, eradication doesn’t mean the job is finished. There are still critical maintenance activities that must be performed to ensure that, once eradicated, polio stays at bay. “Polio assets” have targeted disease surveillance and laboratory support, which could be at risk of getting deprioritized or underfunded in the absence of “polio” funds.
I’m optimistic that we can all learn from GPEI’s transition experience. Here are three reasons why.
- GPEI has a transition plan to help support the integration of “polio assets” into already-existing programs and is acting on it before eradication has been reached.
- An independent monitoring board is providing oversight to the transition process, ensuring regular performance evaluation is ongoing.
- The transition process includes documenting and sharing lessons learned about the initiatives’ successes and failures, including those learned during the program shut down.
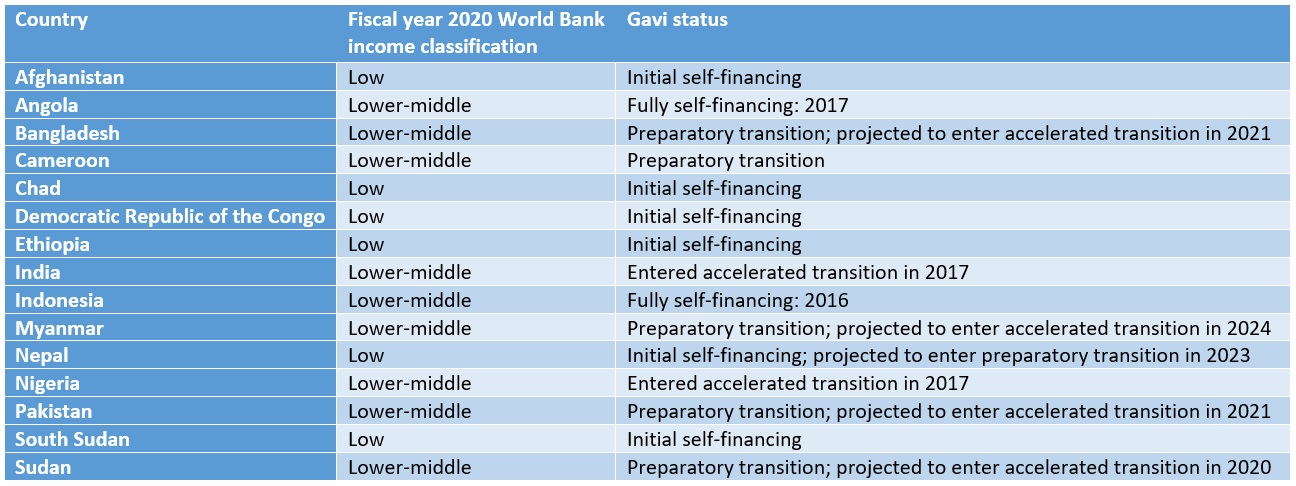
However, I’m alarmed by one of the assumptions GPEI makes regarding transition: that other donors may help fill the gap in “polio asset” funding and provision. In a landscape where other donors are focused on transition, this plan seems unrealistic, hopeful, or at least unsustainable. For example, most of the 16 countries that receive GPEI funds are lower-middle income countries, (i.e., those that are also most likely to begin transitioning out of other multilateral health support, such as support from Gavi, the Vaccine Alliance—see Table 1). If GPEI is unable to garner sufficient support from others for “polio assets” post-transition, other donors with similar intentions for their own departures may need to go back to the drawing board.
Table 1: GPEI focus countries and their corresponding income level and Gavi transition phase
About the Author:
Kaci Kennedy McDade (tweets @Kennedy_Kaci) is a Policy Associate at the Center for Policy Impact in Global Health, Duke Global Health Institute.