Healthcare costs are among the largest barriers to accessing health services and achieving universal health coverage (UHC) in Mongolia. In 2014, 0.7% or 5,681 households in Mongolia experienced catastrophic health expenditures due to out-of-pocket (OOP) expenses, spending more than 40% of their household subsistence income on health care.1 In this blog, I discuss the origins and impacts of these OOP payments, potential policy solutions and their likely impacts, and the challenges that Mongolia is likely to face in tackling OOP expenses in the future.
How Mongolia’s health system has evolved since 1990
Since the early 1990s, when Mongolia transitioned to a market economy, the Mongolian health system has undergone a number of healthcare financing reforms, gradually moving away from the centralized, state-controlled “Semashko-style” model.
In 1993, Social Health Insurance (SHI) was introduced as part of a larger social security reform. Mongolia has achieved high coverage of SHI, with nearly the entire population covered, regardless of their socioeconomic status (by 2014, coverage reached almost 100%).
Primary health-care services, which are vital to population health outcomes and a core component of sustainable health systems, are more easily accessible since they are available free of charge and funded through the state budget.
At present, the current health system is financed by a combination of the tax-funded system, SHI, out-of-pocket (OOP) payments and a small amount of private health insurance. However, Bayarsaikhan and colleagues have shown that since the introduction of SHI, the social health insurance fund (the SSF, or Social Security Fund) has played a steadily declining role in financing health. They note that this “overall declining and unstable role of health insurance in public health financing” has led to a sharp increase in OOP payments. These take the form of co-payments for healthcare services and medicines covered by SHI and user fees for healthcare services and medicines that are not covered either by SHI or the tax-funded system.
In an attempt to move towards UHC, the country is planning to increase the level of financial protection for the population. The government also aims to ensure sufficient funding is available for public healthcare and aims to improve the quality of care by introducing incentives for public hospitals (i.e. supply-side incentives).
Policy context
In the 1990s, OOP payments made up only a small proportion of total health expenditure, but by 2014, the proportion reached 42%. This percentage of 42% is high compared to the countries in the Asia and Pacific Region, and exceeds the WHO recommended level by 17 percent. Such a high level of OOP expenses for health care can have two negative impacts. First, it negatively impacts the living standards of people, causing catastrophic and impoverishing spending. Second, it deters people from using services, simply because they cannot afford direct costs (e.g., costs for consultations, medicines and laboratory tests). Poor households are likely to sink even further into poverty because of the adverse effects of illness on their earnings and general welfare.
Existing policy
To address the high OOP costs that are leading to catastrophic health expenditure, the government of Mongolia endorsed a health financing strategy for 2010-2015. There were some flaws in implementation and monitoring, and the strategy had mixed results. The contributing factors for negative results included lack of evidence and limited understanding of the national health financing strategy by the key policy makers.
In 2017, the Ministry of Health made another attempt to improve the national health system through a new state policy on health. The main goal of the policy was to extend the average life expectancy of Mongolians by improving the quality and inclusiveness of healthcare services. The policy focused on disease prevention, introduction of new technology for evidence-based diagnostics and treatment, and improving health sector financing. Health sector financing aimed to focus on eight objectives, one of which was to reduce OOP costs. The government aimed to keep OOP spending to within 25% of the total health expenditure to increase the level of financial protection for the population in Mongolia.
Policy impact
The average amount of money spent per each household for health as OOP expenditures increased four-fold in real terms from 2009-2014. This is mainly due to the increase in income, improving the capacity per household to spend more on healthcare. However, the percentage of OOP expenditures for health as a share of total household expenditure decreased from 2009-2014.
Changes in some areas of health financing policy also contributed to the decreasing share of OOP from 2009 to 2014.1 For example, from 2010, the ministry of health has used the 115 diagnostic related groups to pay hospital inpatient care, diagnostics and palliative care from the SHI. From 2010- 2013, the number of services covered by SHI increased and the payment rate by SHI for each of those services also increased. Most importantly, essential medicines have been made more accessible by increasing the number of private pharmacies contracted by the SHI. Accordingly, the SHI payment allocation for essential medicines doubled from 2009 to 2014.
Remaining challenges for Mongolia in reducing OOP expenses
Looking ahead, there are three major challenges in tackling the problem of high OOP expenses in Mongolia: the high cost of medicines, the high cost of in-patient treatment, and the high costs incurred by wealthier households.
High cost of medicines
The largest share of OOP health expenditures among all income quintiles is spent on buying medicines. The share spent on purchasing medicine is higher for the poorest quintile than for the richest quintile (Figure 1). The poorest quintile of the population has probably been practicing self-prescribing of medicines as an alternative to seeking services at health facilities (medicines can be purchased over the counter at pharmacies, which are all private).
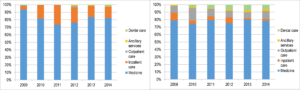
Figure 1: Composition of OOP health payments among the poorest quintile (left figure) and richest quintile (right figure)[Source: Mongolia Household Socio-Economic Surveys, 2009-2014]
However, it is important to note that there is a general pattern of high levels of use of medicines among all income quintiles of the population, for at least three main reasons. First, there are some medicines for health conditions such as TB, late stages of cancer, mental disorders, and diabetes that are in theory fully covered by the government budget, but in practice not all medicines are covered. Coverage is fragmented, and the absence of a strong purchaser system has led to ambiguity between covered and non-covered medicines allowing space for pharmacies to manipulate prices and medicines provided. Second, due to poor coordination among government regulatory and inspection institutions, the mechanisms to regulate drug prices charged by private pharmacies are weak in Mongolia. Third, culturally the perception of good quality care among the population is related to a high level of prescribed medications and injections. Therefore, patients show increased preferences for medicine over prevention and managing life style factors.
High cost of inpatient care
The second highest proportion of OOP expenses is spending on in-patient care (Figure 1). There are two contributory factors related to the high OOP costs of inpatient care. First, despite a policy to exempt vulnerable people such as children and the elderly from any types of copayments, highly impoverished communities still incur OOP health payments. Second, unregulated informal payments are still common in the health sector. One study found that about 60% of OOPs were informal, most of which were paid for surgical, cancer, and maternity-related conditions.2 Technically, health services for these cases are covered either by the government budget or the SHI.
High costs incurred by high-income quintiles
The World Health Organisation defines catastrophic health expenditure over 40% or more of household income capacity used for health services. In Mongolia, households from both higher and poorer income quintiles experience catastrophic health expenditure (Figure 2) due to different reasons. Households from higher income quintiles prefer tertiary, private, or overseas hospitals. Therefore, they spend over 40% of their income on health. However, this does not cause impoverishment for wealthier households. Although the poor spend much less than the rich on health in absolute terms and have less access to secondary and tertiary hospitals they also spend over 40% of their household income on health. In contrast to the rich, the poorer households face a higher risk of impoverishment due to OOP expenditure (Table 1).
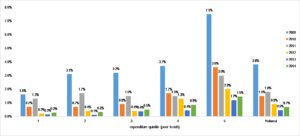
Figure 2: Distribution of households’ catastrophic health payments by income quintile, 2009-2014 [Source: Mongolia Household Socio-Economic Surveys, 2009-2014]
Although it might not be realistic to place restrictions on those who travel abroad seeking health services, the government can work to improve the quality of health services domestically to increase confidence in the domestic health system.
Table 1: Distribution of household impoverishment by total out-of-pocket payment
| Expenditure quintile | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 |
| 1 | 0.0% | 4.0% | 4.1% | 2.7% | 1.8% | 1.82% |
| 2 | 7.0% | 0.3% | 0.7% | 0.1% | – | 0.06% |
| 3 | 1.1% | 0.1% | 0.1% | – | – | – |
| 4 | 0.5% | – | – | – | – | – |
| 5 | 0.4% | – | – | – | – | – |
| Total | 1.8% | 1.1% | 1.2% | 0.6% | 0.4% | 0.41% |
Source: Mongolia Household Socio-Economic Surveys, 2009-2012
The road ahead
To address the challenge of OOP expenses causing catastrophic health expenditure, the government of Mongolia should take two key steps. The first is to strengthen gatekeeping, which is currently weak. The health system has difficulties in controlling self-referrals to higher-level facilities such as hospitals. People from richer households tend to bypass the primary care level, going straight to secondary or tertiary hospitals. Second, SHI coverage needs to be expanded. It currently does not cover all inpatient services in hospitals, and the insured person has to pay 10–15% in copayments to obtain services. In addition, 40% of inpatients pay for the drugs and injections they need during admission.
The increasing level of OOP payments directly affects the socio-economic conditions of the population, especially affecting the poor. Thus, the government must act with a sense of urgency to address the problems identified above.
References
1. Tsolmongerel Ts, et. al. (2017). Household catastrophic and impoverishing health payments in Mongolia. Ulaanbaatar.
2. Mongolian Public Health Professionals Association. (2011). Informal payments in health sector in Mongolia. Ulaanbaatar.
About the Author:
Munkhtsetseg Byambaa is a policy fellow at the Center. She currently works for Mongolia’s Ministry of Health in the Department of Policy and Planning and is the officer in charge of health economics and financing policy.